


Erectile dysfunction (ED) is common — but treatment isn’t one-size-fits-all. This doctor-led guide explains how shockwave therapy and PRP (P-Shot) work, who each option may suit, and how we decide what to recommend first for patients seeking discreet ED care in Luton and the surrounding areas.
Introduction
Erectile dysfunction (ED) is common, treatable, and—importantly—often multi-factorial. In clinic, the best results come from matching the treatment to the likely driver of symptoms rather than choosing what sounds most advanced.
Two options patients frequently ask about are shockwave therapy (Li-ESWT) and PRP injections (often called the P-Shot). They are not the same treatment. They work via different mechanisms and suit different patient profiles.
This is a doctor-led guide to how each option works, whether it’s suitable for everyone, and how we typically decide what to recommend first—particularly for men seeking discreet care in Luton, including the wider Bedfordshire and surrounding areas.
ED is not one diagnosis
ED is a symptom, not a single diagnosis. Blood-flow factors, nerve signalling, stress response, hormones, sleep, alcohol intake, medication effects, and cardiometabolic health can all contribute.
That’s why a premium medical approach starts with a structured assessment: timeline (sudden vs gradual), quality of morning erections, libido, exercise tolerance, medical history, and risk factors (blood pressure, cholesterol, glucose control, smoking). The aim is not to over-medicalise—it's to choose the safest and most sensible first step.

How shockwave therapy works
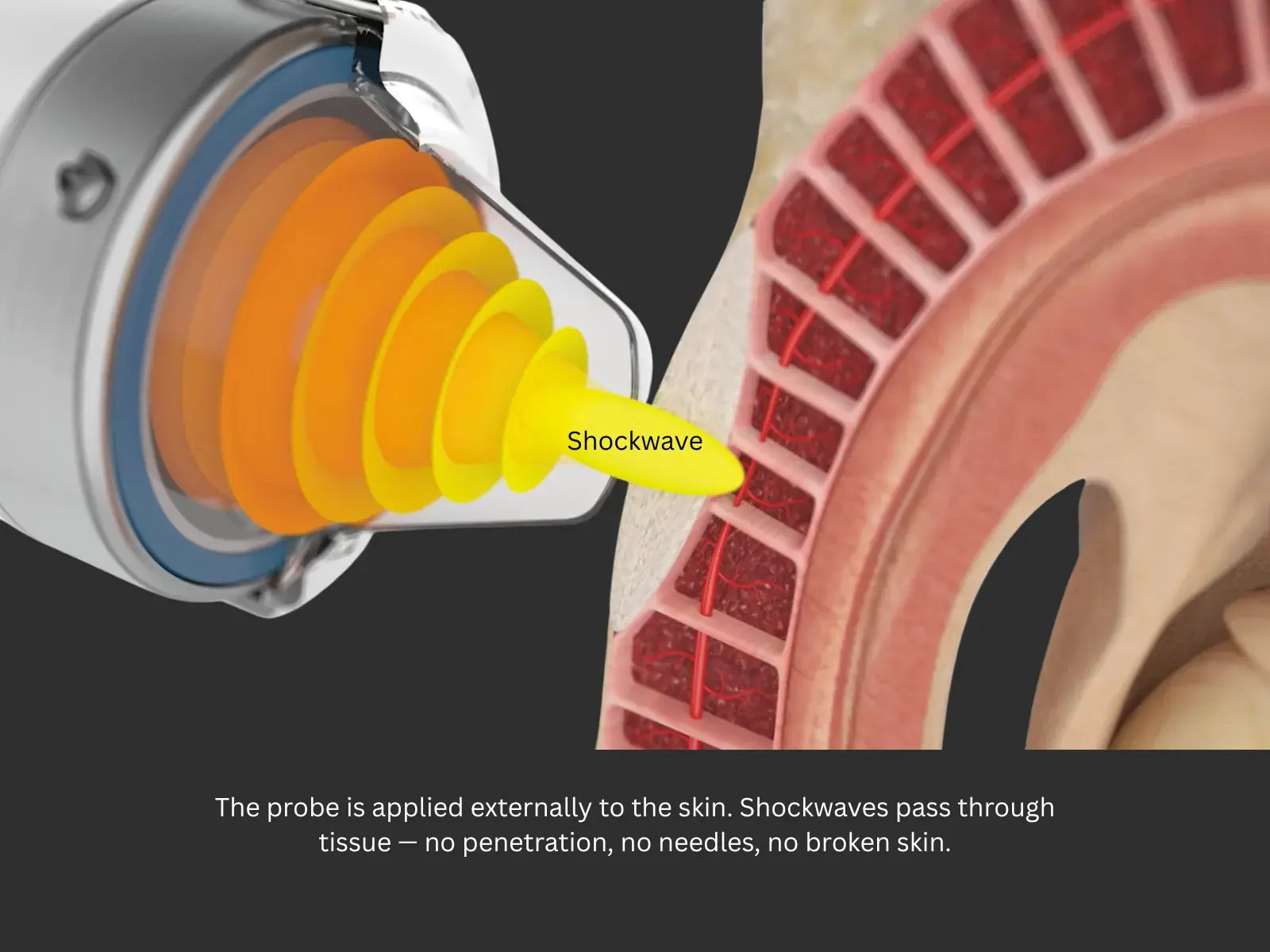
Low-intensity extracorporeal shockwave therapy (Li-ESWT) uses controlled acoustic energy delivered to penile tissues. It is non-invasive and doesn’t involve injections.
Clinically, shockwave is best thought of as a tissue rehabilitation approach. The aim is to trigger biological signalling linked to microvascular function and tissue remodelling. For many men—especially where vascular factors are likely—improvements can build gradually over time.
Shockwave technology has also been used in other areas of medicine and musculoskeletal care, which reassures some patients that it is a well-established treatment modality—although protocols and evidence vary depending on the condition being treated.
Treatment is usually delivered as a course of sessions, with outcomes assessed over weeks rather than days. Device quality, protocol and patient selection matter.

No—and being clear about that is part of responsible, high-quality care.
ED can sometimes be an early marker of cardiovascular risk. Men with red-flag symptoms (for example exertional chest pain or marked breathlessness) should be appropriately assessed. Similarly, penile pain, significant curvature concerns, or other complex symptoms should be evaluated before proceeding with procedures.
Hormonal factors may be relevant when low libido, fatigue, or other endocrine features are present. A doctor-led pathway ensures treatment is personalised rather than package-based. It also ensures the “how” is taken seriously: shockwave outcomes can vary depending on device quality, energy settings and application technique, and PRP results can vary depending on preparation method and injection precision. High standards, clear protocols and follow-up review are not extras—they are central to safety and outcomes.
Shockwave: benefits, convenience and downtime
One reason shockwave therapy is often a popular starting point is its practicality. It is non-invasive, does not involve injections, and most patients can return straight back to normal activities the same day. There is typically minimal downtime, and the treatment course is structured and predictable, with progress reviewed over time.
Shockwave is generally well tolerated, but it is not for everyone. We assess suitability carefully, and would usually delay or avoid treatment in situations such as active genital/urinary infection, significant open skin lesions in the treatment area, or where there are serious underlying concerns that need investigation first. For men with current or recent cancer, implanted devices, or complex medical histories, we tailor recommendations based on individual risk and medical context.
For many men in Luton and Bedfordshire who want discreet, doctor-led care with minimal disruption to work and daily life, shockwave can be a sensible first step.

How PRP (P-Shot) works
PRP stands for platelet-rich plasma—a concentrated portion of your own blood containing platelets and signalling proteins. After a blood draw, PRP is prepared and then injected into specific penile tissues as part of a doctor-led procedure.
The rationale is that PRP may support local tissue signalling involved in repair and regeneration. In real-world practice, patient selection and technique matter, and results can be variable, partly because ED has different causes and PRP protocols differ between clinics. The way PRP is prepared (concentration and handling) and the precision of injection technique can make a meaningful difference to comfort, safety and outcomes.
In a premium setting, PRP should be positioned honestly: it may be helpful for selected patients, but it is not a guaranteed outcome and it is not a substitute for assessing underlying drivers.
When combination therapy can be appropriate
Combination approaches can make sense when:
Combination therapy should never be sold as “more is always better.” It should be recommended only when the rationale is clear, consent is informed, and expectations are realistic.
Luton and surrounding areas: discreet doctor-led care
Many men prefer to manage ED privately, without feeling rushed or “sold to.” A calm, clinician-led environment matters—especially when the subject is sensitive.
What matters most is not a sales package but a doctor-led pathway that includes medical assessment, clear explanation of options, realistic expectations, and follow-up. ED treatment should feel professional and personalised, with suitability and safety taken seriously.
For patients in Luton, and surrounding areas such as Dunstable, Harpenden, Hitchin, Hemel Hempstead, St Albans and Bedfordshire, a discreet consultation can be the simplest way to clarify what is most likely to help first.

What we recommend first: a simple decision framework
The question is rarely “Which one is better?” It’s “Which approach is most appropriate to start with for your type of ED?”
In clinic, we broadly think about ED in terms of the likely dominant driver — for example vascular factors (blood-flow signalling), smooth muscle tone/penile tissue function, plaque-related change, or metabolic and lifestyle influences (such as glucose control, cholesterol, weight, sleep and stress).
From there, treatment is selected in a patient-centred consultation based on medical suitability, goals, and the balance of benefits vs downsides. For many men, this means starting with the option most aligned to the underlying pattern, then reviewing response and adjusting the plan rather than committing to a fixed package from day one.

Key takeaways
FAQs
Is shockwave therapy painful? Most men find it tolerable. Discomfort is usually mild and sessions are quick.
Is PRP (P-Shot) safe? PRP uses your own blood product, but injection procedures can still involve risks such as bruising, swelling, discomfort, and infection risk. Technique and aftercare matter.
How soon will I see results? Shockwave outcomes tend to build over weeks. PRP responses vary—some notice changes earlier, others more gradually, and not everyone responds.
Can I do both treatments? Sometimes, yes—when clinically appropriate. More treatment is not automatically better.
Do I still need tablets? Some men do; others don’t. A doctor-led plan may include medication optimisation if appropriate and safe.
Is ED ever a sign of another health issue? It can be. ED may be associated with cardiometabolic health, and assessment is part of safe care.
Closing
If you’re choosing between P-Shot and shockwave, the highest-value first step is a doctor-led assessment and a plan matched to your physiology and goals. The aim is not hype—it’s reliable function, confident decision-making, and safe, structured care.